Review Article - (2019) Volume 9, Issue 4
Third eye model: a hypothesis to span the diversities of psychiatry and normalcy
- Corresponding Author:
- Kishor Kunal
All India Institute of Medical Sciences
Jodhpur, Rajasthan, India
Abstract
ABSTRACT
Objectives: To formulate a model to define and explain basic characteristics of all psychiatric disorders and normal behaviour
Methods: Analysis of available models, articles, case reports and psychoanalytic reports to formule one common model as per objective followed by explanations of regular characteristics of behaviour, psychiatric disorders and paradoxes
Result: A hypothetical “third eye model” can explain the normal well being, abnornal well being (personality disoreders), normal response to stress (such as sleep, anxiety, fear etc) and abnormal responses to stress (spectrum of psychiatric disorders including suicide and its paradox). Also it can help formulate four laws of psychiatry and various principles which can in turn explain risk factors, criteria for diagnosis, age of onset, duration, clinical features, co-morbidities, risk of suicide, prognosis and evidence-based pharmaco and psychotherapies.
Conclusion: “Third eye model” is solely capable of describing the regularities and irregularities in classification of disorders and their characteristics along with normal behaviour including sleep and dreams.
Limitations: The paper does not include discourse on independent pathways in brain. Also considering the word limit, the author has tried to be precise (not including examples in many cases) and has eliminated the use of explanation wherever deemed unnecessary
Keywords
Laws, Principles, General psychiatry, Etiology, Neurophysiology, Suicide, Sleep cycle, Neuropsychiatry, Dreams, Properties
Introduction
For long, there has been fascinating quests to delve into deepest depths of the mind. With many scientific discoveries, we have come to know about various disorders of neuroscience but one section has always been left behind with the rationale that the section covers a group of functional rather than organic disorderspsychiatry. Many attempts have been made to correlate the neuroscientific evidences to various psychiatric problems but the scientists have often failed to explain all with a single theory. In this regard psychiatry has come to a standstill i.e., when it comes to explaining things with a single model.
DSM-5 introduced the concept of spectrum [1] and that made everything go back to square one because till now we had just classified every disorder and now it was suddenly a spectrum. Interestingly, everything falls under a spectrum. We just need to understand that how it works and it can do wonders in understanding of not only the field of psycho-pharmacology but also and especially psychotherapy. In the following paper, this spectrum has been explained and how it endorses both psychoanalytic model and the neuropsychiatric model. From a normal person’s sleep to the delusions and negativity of a schizophrenia patient-all can be explained in a single shot. Yes! They all can be. And we are not just talking about disorders; we are talking about the gamut of personalities and also about vulnerabilities of the old and the young. The following pages will unravel the history of mind leaf by leaf and it will justify every single act and inertia of a person-wake or asleep.
Materials and Methods
A thorough research of scientific data, case reports and psycho-analytic reports was done. The search was done online on PubMed, Google Scholar, Research Gate along with textbooks and DSM- 5 manual. An attempt was made to formulate a hypothesis which can not only justify both approaches to psychiatry but at the same time explain risk factors, criteria for diagnosis, age of onset, duration, clinical features, co-morbidities, risk of suicide, prognosis and evidence-based pharmaco and psychotherapies. With the help of above material, a hypothetical model was created that was further used to describe various disorders (a brief description has been included in form of supplementary file due to paucity of space).
Results
The hypothetical model (Third Eye Model)
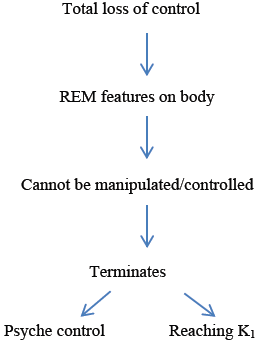
The model has been named such on basis of its iconic resemblance with the “the third eye of Lord Shiva” of Hindu mythology. Now let’s come to the model. The brain functions as a single unit. The role of psyche (the acculumation of conditionings, rationality and intelligence that is acquired over a lifetime) is to control the brain in wake state. Before understanding the wake state, we shall endeavor to understand the sleep that symbolizes the activity of uncontrolled brain. Also we must understand that the brain here is just an organ with advanced functions and like any other organ its working area is defined. The flow of work is as shown in (Figure 1).

Figure 1:Is the sleep cycle with neurotransmitter theory. Outer circle represents the level of SE/NE which is directly proportional to brains activity as we can see from the cycle. There is no psyche so nothing to control the inner circle. K1 and K2 are artificial points denoting the highest and the lowest levels of SE/NE activity in brain.
The exhaustion marker of brain is defined by high SE (serotonin)/NE (norepinephrine). When SE/NE reaches its max it activates a point “K1” in the cycle. As soon as the K1 point gets activates it initiates a process “Y” that will start mitigating the activities of brain, thus also reducing the production of SE/NE probably as a protective measure. This “Y” process continues until the SE/NE falls to its lowest ebb in turn activating “K2”. In order to protect itself from falling into coma or a vegetative state the brain needs to start functioning again. This is what happens at K2. At this point another process “Z” will get initiated and that will activate the brain (increasing SE/NE) and thus mimicking the wake state. In sleep state there is no psyche part to check the flow of this cycle so, the cycle will continue without having even a pint of consciousness, and, since the brain is mimicking the wake part and its work increasing- the SE/ NE will increase until the zenith of the threshold for the brain, again activating the K1 point and continuing with the Y process. The cycle from K1 to K2 can be considered as NREM phase and vice-versa as REM phase [2-5]. In other words, higher serotonin/norepinephrine will correspond to tiredness in a flow (only case where this is high other than wake state or tired state will be the initiation of rest/sleep)
When the brain is mimicking the wake state it will activate the areas that are necessary for functioning in wake state. This will trigger the memory and thus the conditioned reflexes and since psyche is still asleep (not checking the function of brain) and the show has to go on; the brain follows a very basic path of the point shifting model (explained later in properties of dream). While shifting from one point to another the brain can randomly choose any conditioned string for that point. This string can either be a deliberate sequence of events or a simple binary string (having one start and one end point). The deliberate sequence can be responsible for repeated nightmares and the random binary strings for bizarre dreams. The number of strings stored in memory for any point can be variable but once formed it stays unless de-conditioned or reconditioned. Since the brain is mimicking a real world it creates a scene in space during this point shifting process. The eye moves in order to visualize these points in space. The eye will move because it’s seeing those points in reality. The quickness and randomness in pointshifting, is what makes our eye movement very random during this part of sleep. If we are seeing a nightmare it may happen that our body also moves as a protective response
On waking up
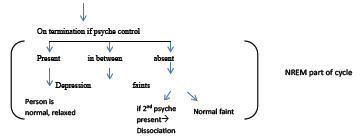
As soon as we wake up which is most likely at the point ”K1”, the psyche inhibits this whole process and there is a constant struggle between the brain and psyche where the brain is trying to continue the cycle and psyche trying to check the cycle at whatever point it can. Like, we are tired and feel sleepy because the brain is trying to simulate the NREM part of cycle (similar to Newton’s first law of motion) and our psyche is controlling it till we start feeling wake again (REM part of cycle) or else we will give up to brain cycle. The feeling of mental exhaustion and excitement is a part of basic cycle of brain while our psyche is just trying to use our brain in order to make it perform its desired activities. The conscience and prudence are properties of psyche (anything acquired is a property of psyche) and thus when the psyche is inactive (during sleep) we have no conscience or prudence (there is no logic in dreams) until that has been conditioned. The activity of brain during a life time is almost unchanged except for fixed and predictable changes in duration of REM and NREM, it is the activity of psyche that changes from childhood to old age and this will define the distance between two parts of the cycle in model. The more we train our psyche the more the lids of the “thirdeye” come closer (inner circle converts to oval), and the more it comes closer the more we are able to control our brain and the more we are able to so called behave (or misbehave if the psyche is made that way- explained later under discussion on types personality disorders) while being wake. In normal wake state the brain cannot continue with this cycle because the psyche is constantly checking (LAW 4 explained later) it but if due to some reason the psyche stops functioning (during sleep or during stress in wake state) the brain will continue with its cycle. That is why in normal adult individuals this cycle can only be present during sleep or in flashes during the wake state (when due to some reason like exhaustion the functionality of psyche is reduced). However during stressed state, when the control of brain cycle by psyche is partial or inadequate, the response would be somewhat unpredictablethat is where the psychiatric disorders come in. Interestingly enough, one can adequately deduce, which disorder will occur in a given individual based on the algorithm (Figures 2a-c).

Figure 2(a, b and c):(in horizontal order) are (b) Variations of “The third eye model” (c) Shows normal individual.
Discussion
Sleep is the mirror of self. Dreams are what we see in the mirror. The discussion here aims at formulation of the working model of brain and how it manifests in both wake and sleeping state. This discussion has two parts as we seethe physical laws of psychiatry and properties of dream. The properties of dream have been discussed first followed by formulation of physical laws of psychiatry and derived principles. The hypothetical “third eye model” has been already explained in the results section. Based on above, an algorithmic approach to psychiatry has been created. The answers to many questions-such as what forms the basis of psychotherapy and pharmacotherapy- follows along with reasons for age of onset and duration of untreated domains of disorders. It is followed by the explanations for some regular happenings in normal life followed by a brief diagramatic representation of personality disorders. All of which is followed by detailed analysis of various disorders based on formulated laws and algorithm.
Properties of Dreams
Point shifting
The dreams move from one point to another. It is similar to moving from one scene to another like in movies only difference being that here the scenes is only connected at end points. For this I would like to take help of a little illustration (Figure 3).

Figure 3:Is called the Point-Shifting model. There are 4 sequences in this example: A to B to C, C to N, M to N, E to F with M. Note most of them are in binary format but some are deliberate which can be combination of more than or equal to 2 binary data. We go from one point (A) to another (B) and to another (C) to which we relate a point from another memory (N) which was also related from another point (M) and then the mind finds out that this new point is actually also stored in some other format (with F) and from there we could reach the last point (E).
Propagation
Propagation follows the principle of inertia. Once started and given ample resources, the dream must go on no matter what you see. This propagation is assisted by two properties of dream that I will explain in following points-non-inhibition and randomization. As known from point shifting property, the propagation will use- as its resources- the conditions or strings stored in memory- which will be further explained under the property of “exposure and conditioning”. For ending the dream the brain must stop this propagation and for that it will have to snatch away the resources by either interrupting the supply of neurotransmitters or by being alert.
Disinhibition
During sleep state the intelligence and semantic memory is given rest so the flow or propagation of scene(s) is unchecked and what we see is nothing but wake state minus the sum of rationale and modesty (the two characters of a so called sound and civilized person)-broadly-the awake person minus psche.
Randomization
The principles of randomization come wherever there is free will and since here is Disinhibition, the randomization will be there. The principles are known to everyone. It is the same randomization we use to study in statistics. The probability of getting a sequence after another is same for every sequence stored in brain related to that particular point. At this point we can define dream as reality minus psyche and that would mean that they represent the bare brain cycle with its profound data base.
Impact and Conditioning
Impact
Anything which on exposure makes an impression on our mind in known or unknown terms is termed as impact. Now in our memory the data is stored on “First come-First serve basis”. Anything that comes first in relation to something is stored with that thing in the binary format but the condition is that it should make a literal ‘impact’.
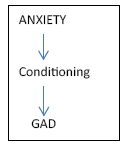
Conditioning
Formation of a string in response to an impact is known as conditioning. The brain processes whatever data it is given and stores the one which makes an impact in a form of string with the points being what have made an impact (not every sequence of reality will make an impact so not everything will be stored in the string). Similarly, anything seen in a dream can also be mistaken as truth especially in childhood (because there is less information of social norms and scientific reasons) and they can also be conditioned if they make an impact just as that would have made an impact in real life (forming a base for dissociation-explained later).
Like in the example of point shifting, the conditioning from the dream could be like this (Figure 4).

Figure 4:Means that the brain can store any information from these sequences as it pleases (or as impact is made) and from anywhere to anywhere under conditioning. This is not just for dream but even for real world phenomenon. The conditioning here simply means that if point A comes in a scene, anything from a set of (B,C,N,M,F,E) could come next or anything from a bigger set like {(B to C to N to M to F to E), (B to C to N to M), (B to C to M)…………} could come if it is being deliberate. This also means that a continuum of binary strings can condition into a deliberate sequence and from a deliberate sequence we can get a number of binary strings.
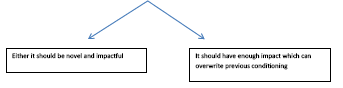
Summarizing this property, any exposure which leaves an impact is conditioned. The conditions are stored as strings where one has to precede or succeed the other-the sequence is immaterial. The conditions are formed on “First come- First serve” basis so most of them are formed in childhood and many may not even have a sound meaning as these may include superstitions and many cultural practices. The exposure as mentioned earlier could just be in form of an idea-material interactions are not necessary. For clarity, if a person sees, hears, smells, touches, tastes or feel anything that is counted as an exposure. Also, if a point B is stored in relation to A, it is said to be conditioned to A and vice versa. All these conditioned responses can be replaced/removed/subsided depending upon impact of creation of new one following survival of the fittest philosophy which also means that if the impact of older one is more, new ones may not be formed.
Till now we have understood that the activation of a conditioned memory from dreams or reality into a dream but if in any case, the episodic memory (conditioned memory) from dream is activated in a real world by seeing something in reality that could have been a result of randomization in dreams it can lead to feeling of DÉJÀ VU. It also explains why sometimes serendipitous discoveries occur and most of the times it doesn’t. Dreams can give a person a fresh perception of his theories. His thoughts due to their high frequencies are conditioned in binary formats which in process of randomization can result into a new discovery because brain is not biased in point shifting- so a discoverer can actually see a sequence in dream which he would not be able to see in reality.
Bereavement reaction can be examples of increased amplitude leading to impact. Deconditioning by social interaction over weeks to months can make a person social again but it is not possible to recover completely resulting into dreams of the deceased even after years of end of bereavement reaction. This can also explain “war neurosis”. Similarly anxiety is an example of increased conditioning and continues until it is de-conditioned. Any anxiety/grief can be eliminated by a simple nap if not conditioned. Also, we can understand that any repetition in dreams is either because of increased conditioning or it can be just random co-incidence.
Since children are not much exposed and thus not much conditioned, they are liable to have static and bland dreams -a conclusion that is very consistent with findings of Foulkes [2].
Jung argued that the archetypes of the collective unconscious express themselves through a set of inherited symbols that also appear in myths, religious ceremonies, and other waking practices. Conditioning property could be responsible for that [3].
This also supports the conclusions drawn regarding properties. Since most of our encounters are made in childhood only, we make first impressions and thus conditioning is done mainly in childhood only. Later on, only an impact of greater amplitude or frequency could over-write it so chances of having changes in dream content is reduced. Also, with age, rationality and modesty comes and thus a frequency of such conditionings could over-write the earlier conditioning leading to decreased aggression and negative emotions. Also, a reduction in conditioning can occur with older age due to very high number of inhibitions in daily life (physical, rational, emotional and social) thus increasing the number of bland conditioning. This could be a reason of conclusion observed by Abel [4] and Giambra et al. [5] a decline in dream reports with age. Similarly if one has higher memories from childhood (the conditioning from childhood has lasted long) and thus can remember more dreams- a correlation found by Schredl et al. [6].
While, Hall [7] and Lakoff [8] argued that the unusual features of dreams, such as unlikely juxtapositions, metamorphoses, and impossible acts, may be the product of figurative thought. The dreams can actually be so as it is randomized and non-inhibited.
Randomization property of dreams can be supported by various researches such as that of Kahan [9] finding that 60% are completely unaware of dreaming while in a dream, and that 46% were completely unaware of controlling any aspect of the dream experience and Foulkes [10] subscribing to the notion that night dreams are generated by spontaneous brain activity during sleep. Not only the researches, this can be supported by the fact that we get a lot of bizarre dreams. The chances of getting a dream can be increased or decreased by randomization principles. Randomization is indeed helpful. It can be used for getting off the dream. If you are having a nightmare and you counsel yourself to break the dream or someone wakes you up it breaks the flow and the next probability of having such a dream would be very low thus shooing your nightmare off but a permanent treatment would always be de-conditioning.
Both continuity and compensatory roles can be explained as dreams are non-inhibited they can show some characteristics which we have suppressed in real life-showing what Jung might have thought as compensatory. Also, the latter can be explained as the ones having more of abnormal or non-inhibited actions in real life are likely to have formed such conditionings in brain (as explained under first come first serve basis). Quiet interestingly it can also explain the metaphorical representation in dream like when the mind is shifting from one point to another it cannot differentiate between two different meanings that an end point could mean. Like a “back” could just mean a body part or the back of someone. This is actually the result of the synergistic effect of a sleeping semantic memory and hyperactive conditioned responses.
Sleep: The bridge of “Third-eye” model and laws of psychiatry
Sleep is made up of two physiological states: non-rapid eye movement (NREM) sleep and rapid eye movement (REM) sleep [11,12]. In normal persons, NREM sleep is a relatively peaceful state compared to waking [11,12]. The pulse rate can be typically slowed upto ten beats a minute below the level of restful waking and is regular [11,12]. Respiration is similarly affected, and blood pressure also tends to be low relatively, with fewer variations [12]. Pulse, respiration, and blood pressure in humans are all high during REM sleep-much higher than during NREM sleep and often higher than during waking. Brain oxygen use increases during REM sleep [12]. The cyclical nature of sleep is regular and reliable; a REM period occurs about every 90 to 100 min during the night [12,13]. The serotonergic and noradrenergic system acts as REM off system with cholinergic neurons reaching its peak firing levels in the mid of REM [14,15] The firing of SE/NE neurons increase during the REM phase ultimately turning it off [14].
The sleep cycle is the most undisturbed phenomenon in any brain and thus is almost similar in normal individuals. So, if there is anything that could give rise to a potential hypothesis, this is certainly one of them. Also, now the question arises-how? For this we can make some basic physical laws of psychiatry based on the observed data but the condition should be one- it should act in similar manner for diseased and normal. Interestingly, this can be done based on the below mentioned hypothesis. From the above discussion, we can formulate laws of psychiatry as follows:
Laws of Psychiatry
First law
States that the REM equates activity for the brain and NREM equates inactivity [12].
Second law
States that the affairs of brain run in a cycle of which REM and NREM are two parts [11,12].
Third law
States that the activation of serotonergic and noradrenrgic neurons are responsible for REM activities of brain and their deactivation leads to initiation of NREM inactivity and vice versa [14,15]. (Please note: Cholinergic, dopaminergic, glutaminergic and gabaergic neurons and pathways are connected to them which have been explained in the paper under drugs section)
Fourth law
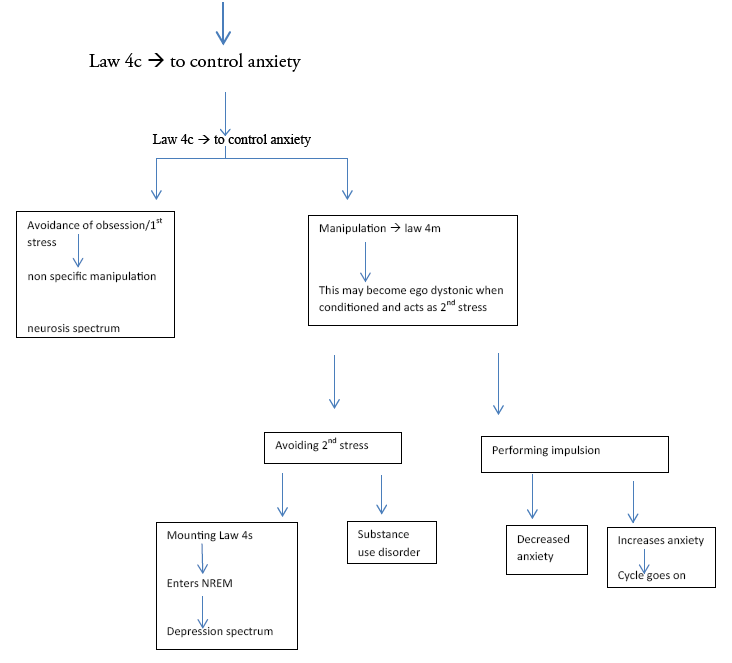
State that the brain cycle can be controlled (4c), manipulated (4m) or stopped (4s) by psyche at any point as per environment requirements and conditioning [16-18].
This means that there is a 3-tier system functioning inside the brain in which the top most position is of psyche which constantly checks the activities of brain cycle (the natural cycle which determines the most primitive status of brain functioning-can be called as the basic unit of brain’s function) and according to the part of the brain cycle in which brain is and the given environment creates a response for the body. This response can be voluntary as in normal life or totally involuntary as in case of panic (explained later with the algorithm) or a mixture of two. So, the 3 tiers are: brain cycle, psyche and the response- in the given order. In sleep state, there is no psyche so body is under direct control of brain thus the manifestation on body (response) is in direct proportion to brain cycle. Controlling (4c) would mean less action (response) as per requirement and termination would mean no action as per requirement in REM and opposite in NREM. Manipulation (4m) would mean actions (response) are not exactly in accordance to requirements. Sometimes a combination of two can also be a manifestation. Stopping (4s) would simple mean cessation of activity or inactivity as per the state of brain. This 4c, 4m and 4s can be present independently or simultaneous with each other. Like, to go into an active state from inactive state (as in going from depression to mania) the psyche would have to control the response of inactivity (4c), and then stop the response (4s) followed by or along with some manipulation (4m). Though this might seem complicated but this is what is being done daily by our brain. Like when you are dozing off studying your response is inactivity but you have to study so your psyche instructs the brain to stop sleeping (4s) and either you simply control your sleep, dozing off less frequently (4c) or indulge in some activities that your psyche might think-will change the response as in washing your face or hearing some music or drinking water (4m).
This leads us to formation of a model (as discussed earlier) and a few principles in accordance to above mentioned laws.
Derived Principles
Principle of least (N) REM duration
Least (N) REM duration will be when control by psyche is absent completely.
Explanation: this situation occurs in sleep and in panic. But there is a difference between the two. In dream the cycle goes from K2 to K1 in REM, thus denoting the maximum time stayed in REM in absence of psyche’s control. This time can be given a multiplication factor of 1. In presence of even a little control, the psyche would increase this factor. In panic the psyche follows this path but from a point between K2 and K1 to K1 so the time duration of panic could not exceed the maximum time of REM. Also in case of bipolar disorders, the pace of the cycle can be determined if we know the duration of either of mania or depression. By law 4, we know that psyche controls REM and NREM and we also know from above discussion that control by psyche is lost a little so it will affect the pace of the cycle by equal multiplication factor (M) (Law 2 and Principle of least (N) REM duration). By this we can know that maximum limit of mania is countable in absence of treatment which is 3 months [12].
Principle of definite proportions
The time spent in each part of cycle is different but in proportion (from second and third laws). This principle can be used to determine the duration in untreated individuals of bipolar affective disorders in which we know the duration of untreated mania/depression thus finding out the multiplication factor and then the proportion by EEG studies in the given individuals. eg. Ratio of REM and NREM in the individual at the given time in a proper sleep cycle in EEG is “r” and the duration of REM is “d” and NREM is “dn” and multiplication factor be M. also the duration in real life of untreated mania be D and Depression be DN. Now, from above, we can say:
d/dn=D/DN=r. Also D=Mxd and dn=MxDN
Principle of stress
Stress can be understood as an external stimulus (other than brain cycle-which is an internal stimulus) that acts as a distraction for psyche. So, it is the response of the psyche to stress, continuum of stress and response to the continuum that determines the manifestation of our brain cycle (details are followed in algorithm)
Principle of positive feedback
The progression of each part is by positive feedback until threshold/stopped. From second law, we know it will run in a cyclical manner and will go to other part at point K1 and K2. From fourth law we know that it can be terminated by psyche so by these two we can derive this principle.
Principle of neurotransmission
The activity of REM and NREM is proportional to activities of serotonergic and adrenergic neurons only difference being that, in the former activity is increasing and in latter the activity is decreasing. This is very clear from third law and principle of positive feedback. SE/NE can be seen as fuel for the cycle.
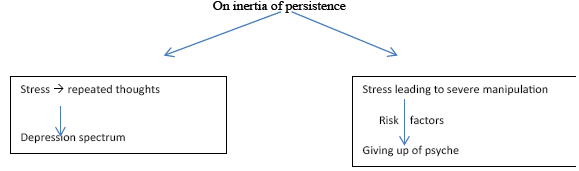
Principle of inertia
A person always tends to be in one state until inertia is broken. This inertia is created as a result of a conditioning mounting a particular state of brain (REM/NREM). This principle is the key in development of diseases. When a person is in a particular state, he will be in it by principle of positive feedback and the psyche will employ conditionings to keep it in the same; leading to inertia unless broken.
Principle of logic
Logic can be used to develop and relate conditionings and thus is only needed and present when psyche is active. Logic will guide psyche and thus development of logic is crucial to moderate behaviour in wake state
Even in dream if the logic is absent, the wake state can use logic to find a meaning of dream. The psyche can for sure use logic but what logic it will use will depend on three factors:
1. Environment
2. State of Brain: REM or NREM
3. The goal it needs to achieve (like in above case it can be just solving a dream or it can be finding a hidden meaning in dream that would shape life or it can just be finding hidden wishes as in psychoanalysis)
Principle of conditioning
The conditioning of responses defines how a person reacts.
This is the most fascinating principle because this forms the basis of psychotherapy. If we anyhow, condition the psyche that talking about stress will calm down the anxiety (a conditioning that is well prevalent in our society but often the person may not find one to who he should talk to), we can eliminate the anxiety by talking about the initial stress. Also if the patient is telling that this particular thing is causing stress and the doctor has talked it out completely without downgrading the anxiety, then possibly there is some other deep rooted stress or the patient is lying.
Principle of personality
The cumulative effect of all conditionings (past and present) in accordance with principle of logic will lead to conditioning of psyche and thus formulation of a personality. An altered personality is the one which is not in accordance with social rules for age, sex and culture and that alteration is being a problem for him or others.
Principle of suicide
A suicide can only take place in a REM state in response to a NREM state.
By principle of logic, we understand that behind every activity and inactivity of wake state there is logic and inertia. Sustained inactivity will lead to formation of new conditioning that will in turn change the psyche of a person (by principle of conditioning and personality). This new psyche can promote a person to die (a permanent/ perfect state of inactivity) only when the person is inactive (principle of logic and inertia) but this in turn becomes protective for the person because he cannot commit suicide which is an activity (but he can commit such suicides where it is not an activity like euthanasia) so for committing a suicide his psyche must enter the REM phase then only the psyche can make REM commit the activity of suicide (by principle of logic). Interestingly by second law, the cycle will go on and by principle of (N) REM duration, we can know that what is maximum time limit in which the person can commit suicide (usually capped at 3 months).
So suicide will need at least following ingredients:
1. A conditioning that death is the permanent solution for rest.
2. An NREM state to incept the idea of permanent resting.
3. A REM state to produce an activity or a plan for conducting the activity.
4. From above discussion we can see that risk will be more in persons who have [12,19].
5. Stronger conditioning: severe depression.
6. No re/de-conditioning: no one to console or to live for (unmarried/divorced).
7. Compelling environment: persistent stress.
8. Fast onset REM: in early stages of recovery from depression.
9. Long duration REM: maximum to a period of 3 months.
We will see the risk of suicide with individual diseases and how the duration of any disease, risk of suicide and others can be calculated at the end of discussion.
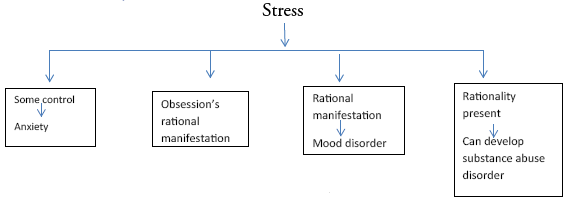
The algorithm of response to stress
Now let’s see what all responses we can have to stress and some prototype diseases. For convenience purpose and to avoid any confusion in diagnostic criteria, different responses have been mapped into a long algorithm (Diagram 1) which have been further divide for ease of reading.
We know by Law 4, psyche controls, manipulates and terminates the activity of REM and NREM by conditioning. So “Reversal of control” needs:- Stronger psyche motivation: (to give upto brain’s cycle)
Person shall be convinced other life is better Person shall have a strong motivation for such things
For paranoid/disorganosed behaviour a stronger REM and very strong conditionings required. For negative/catatonic, less conditioning required.
Person shall not be convinced otherwise (Therefore, a person cannot become a patient of schizophrenia is he is happy, not going through major life problems and is very understanding and content).
This not only explains the age group but also the risk factors for disease.
Weaker psyche structure:-
Else it would counter the reversal of stress
Conclusion on miscellaneous aspects of disorders
Now we will conclude certain points in short.
Relation of age with disease
For any psychiatric disorder to occur the conditioning is a must. The type of conditioning will determine and even predict the disease. At a childhood stage, there is usually no or little conditioning as to why should we die, what does death mean and all so it is less likely to have suicides in early childhood but yes, in early childhood the children develop following coping skills:
Falling down to seek attention.
Getting away from problems could mean running away (metaphorical conditioning). Being stronger and bolder (if presently not) would help coping and this could lead to dissociation if environment doesn’t permit. Being ill could save from some stress.
If you want to hurt someone don’t do what they want (conduct disorders).
These all could lead to conversion disorders, dissociation disorders, factitious disorders and conduct disorders as per the algorithm. This spectrum can continue in adolescence, except that, the fifth one becomes more specific and a few more are added.
Realization of meaning of death and the modes by which it can be achieved.
This could mean that an extra coping skill is gained-suicide. Also in adolescence come many stresses, so adolescence is theoretically the golden age in psychiatry. It will define not only a future being but also how could the person respond to certain stress and how much his psyche is stronger. This along with new conditionings shape the psyche of individuals so many of personality disorders can be diagnosed.
Adulthood would only see the strengthening of conditionings and its uses in coping with stresses. Usually most diseases can present in early adulthood if coping skills are not enough or the stress is too high. By the time one becomes an elderly, the person will not get new conditioning usually, NREM would become prominent and body also gives up so falling into the trap of depression would become easier.
Duration of illness
From above discussions, laws and principles, we can find out some similarities between sleep, normal awake and abnormal awake states. The comparison of a few situations have been given in a tabular form Table 1.
Table 1: Comparison between different modalities presenting in psychiatry
| Early sleep | Late sleep |
|---|---|
| Later life | Early life |
| Immediate response to stress | Adaptation of that response |
| Effect of tiredness | Effect of freshness |
| Total duration is short and variable in individuals | Total duration is longer, fixed and in accordance with first |
| REM upto 10 min in a cycle of 70-100 min | REM 20-25% (18-30 min) in a cycle of 90-120 min |
| Stage 3 and 4 present of NREM | Absent |
| Starts with NREM | Starts with NREM |
For calculation purpose we will use Table 2.
Table 2: Duration of various stages in NREM and REM
| Stage of sleep | First cycle | Percentage of total sleep in night |
|---|---|---|
| NREM stage 1 | 1 -7 min | 2-5% |
| NREM stage 2 | 10-25 min | 40-55% |
| NREM stage 3 | Few min ( usually only first cycle) | 3-8% |
| NREM stage 4 | 20-40 min (usually only first cycle) | 10-15% |
| REM | Upto 10 (1-5 min) min in first and 18-30 min in subsequent cycles | 20-25NeuropsychiatryNeuropsychiatry% |
Now we can clearly see why first panic attack can even go unnoticed and subsequent ones will never last more than 30 min. also we can see that untreated mania usually lasts for 3 months. By table we can clearly see that REM is 20- 25% and NREM stage 1 and 2 is 42-60% this makes a clear interpretation that in first cycle NREM portion is usually more than 85 percent of cycle which gives us a multiplication factor of a 5.67 for first episode of a NREM disorder as compared to REM. However in subsequent episodes REM accounts only for 20 to 25% that makes a multiplication factor of 3-4. So in a treated or second episode of mania lasts for a max of 3 months, the same for depression would be 9-12 months.
Also we see earlier REM state is very short but with time it tries itself to be equal to NREM state and the same happens with mania and depression episodes. Also stage 3 and stage 4 can be considered severe depressions.
By principle of definite proportions, we can know different amount of time spent in particular state and from algorithm, we can map out durations using research data.
Also, an interesting finding in Hindu mythology are the prayers that contain 40 verses (chalisa) known to remove fear after reciting it a number of times (seven as often written in the prayer). For example if you recite Hanuman Chalisa (40 verses of the given prayer of Lord Hanuman), it will take around 13-14 min (average time of panic being 10 min can be overcome by this), so as stated in the prayers that are centuries old, it can scientifically remove panic (control of brain cycle by psyche).
Multiplication factor for a disease (M)=duration spent in disease (Dx)/ duration of stage of brain (dx)
By further research we can find multiplication factor for every disease.
Drugs
The main neurotransmitter is serotonin and it is complimented by Noradrenalin. By common sense we know that when NE falls Ach rises and vice versa so we can clearly see that when NE would start falling after K1, it will initiate a process Y, which in mid-way will excite the cholinergic neurons once NE levels have fallen to a particular level similar when NE will start rising after K2, it will initiate a process via process Z to control cholinergic secretions making theoretically Ach highest in somewhere mid of REM and lowest in somewhere mid of NREM. One theoretical observation is to be noted that since mid NREM has lowest Ach, so if we block the Ach for a long time, the brain would actually simulate mid NREM like feeling and that is why we could feel sedation with antidepressants or antipsychotics or antihistaminic which have anticholinergic properties.
Similarly glutaminergic pathways is an excitatory network which will work in accordance of its pathways in REM and GABAergic neurons are inhibitory ones which can be used for control of excitation. Thus GABAergic neurons can be used for noise control as in panic and anxiety [13]. Also dopaminergic neurons are a part of Z process and thus their activation also leads to various manifestations of activity and REM and they can be controlled accordingly. Their significance is especially in schizophrenia, where person believes in delusions and hallucinations so much that it becomes a part of his new life. By blocking dopamine, we are actually not allowing the brain to see those and thus helping person to come back to his original environment. Also in schizophrenia, the defect is mostly in person’s perception of environment that has led to reversal of control so we can either change the perception or improve the environment, i.e., why family interventions are very necessary.
We also know that if we want to control the cycle we can either decrease or increase serotonin. This will change the levels of serotonin in brain and control the cycle as if the psyche was controlling the cycle. So in any neurosis disorder (psyche is active and tries to mount a response) SSRI would be beneficial because it will reduce the need to mount a full response and symptoms are controlled (but of course the mainstay would be to make psyche control the response). Of course in disorders like panic where REM MF is 1, giving SSRI would initially mimic panic only because it is also increasing it but with time psychotherapy would control stress and symptoms would be controlled once level of SSRI is optimal. SSRI could also be beneficial in those psychotic (psyche cannot mount a proper response) disorders where we need to mount a REM response like in depression. In psychosis, our aim would in fact be to control the REM so we would actually give blockers so that the effect of disease could be mitigated and as mentioned earlier person could be brought back to normal environment. So here we would use serotonin blockers (this controls the brain cycle mostly) or dopamine blockers (uncontrolled REM’s manifestation)
Role of behaviour therapy
When the thoughts are being expressed as actions and when the thoughts are normal in most and actions too except for the fact that here action is increased in amplitude of frequency. For example, wishing to watch pornography to attain gratification makes person watch pornography. This is very normal but if this is increased very much, it can be counted as perversion. So, here behavior therapy can work. Also, in phobia, fear (thought) and being fearful on exposure to known and speakable stimulus (action) is normal but it’s increased in amplitude and frequency is counted as phobia. So, behavior therapy can work. In personality disorder or schizophrenia, behavior therapy alone cannot work because these are multitude of signs and symptoms complexing the therapy.
Whenever there is no manipulation --> no action --> behavior therapy alone can’t control.
Even in cases of manipulation, the behavior therapy alone cannot work (because, though it can control expressed thoughts but it cannot control thoughts leading to expressed thoughts). For example, it can control the “checking” compulsion but cannot remove the obsession behind it. So, with this know where to give just BT and where to give CBT. Personality disorders which include (Figures 5-8).

Figure 5(a, b and c):We can also learn from these that schizoid personality will be a risk for depression while paranoid can be a risk for mania. Schizotypal clearly is a risk for schizophrenia. In schizoid personality psyche is less trained to control NREM state while in Paranoid personality it is less trained for REM state. In Schizotypal, there is combination of two.

Figure 6:Shows obsessive compulsive personality. This personality is prone to develop to compensations and will likely be more anxious if brain cycle is not controlled well like if anything goes against their wish because their psyche is not used to it and it will count as stress. Schizotypal and obsessive compulsive personalities can be seen as opposite to each other in their etiology.

Figure 7(a and b):Both antisocial and borderline personalities have risk to develop psychosis. With psyche functioning in accordance to brain cycle at specific levels, the brain will tend to push the SER states to that level for max coherence. Now this may lessen the conflict between psyche and brain cycle but it also increases the risk of getting psychotic symptoms as a part of daily life and hence also makes them vulnerable for such diseases. Antisocial can easily develop mania of course with mild depression while borderline are more prone to develop severe depression with hypomania thus also explaining suicidal thoughts and tendencies.

Figure 8 (a and b):Can clearly explain that both these personalities are reluctant- one is always and the other to specific situations but they also share one thing. They both can be at risk for developing anxiety spectrum disorders because to any stress the psyche is hyperactive and when brain will tend to have NREM simulation psyche will try to simulate REM. Interestingly their dreams will not suffer because as soon as the psyche is gone brain cycle can run smoothly but yes due to defective psyche they can present with anxiously conditioned dreams and can have more nightmares too. In the first case the psyche would need reinforcement for even a small stress but in avoidant personality as we can see the psyche is trained to be dependent in certain specific situations so the person might feel that he is inferior in only some situation resulting in inferiority complex while in former the person will know he is inferior so no reason to have inferiority complex.
Panic Disorder
Etiology/diagnostic criteria
1. Manipulation of stress not possible.
2. Person ‘wants to control’ stress.
3. REM mounted.
4. Situation ‘should be’ under control.
5. Situation is presently not under control.
6. Stress cannot be told or justified by the person.
7. Situation is totally not controlled [1].
Clinical Features
1. Duration-maximum duration is given by principle of least (N) REM duration. It will be equal to amount (the distance from K1 to somewhere uptill K2 say to a point Kx) of NREM simulated by conditioning with a multiplication factor 1. For explanations see below under duration section of discussion. This is usually capped at 30 min [12] with the average being around 10 min (1 to 18 min) theoretically. In some situation, especially when the person had tried to exercise some control initially, the duration may increase slightly which is practically very possible.
2. Onset-at the rate of brain cycle (within minutes) so uncontrollable [20].
3. Self-limiting (because will automaticity terminates at K1)
4. Features of termination
5. Since, person is awake, the features of REM becomes appreciable and this acts as 2nd stress, (Eg. person can feel having MI) leading to further conditioning of this 2nd stress with the first one.
6. Feeling of intense fear (most gruesome fear on scale).
7. Any feeling that comes in pain will depend upon conditioning (what a person thinks might happen/be happening to him, when his control is lost). For example, if the person thinks he will die of heart attack that feeling will increase.
8. If the person thinks, he is dying and not specific method of death will increase and not any manipulation. So, culture specific symptoms may be seen.
9. Actually, panic is nothing but the person’s perception of REM’s manifestation in body (“Z” process’s manifestations).
10. Risk of suicide: if there is previous depression the risk is high because person is able to mount a good REM and also because there is previous stress which is “not under control”. So, basically in these patients, risk of suicide will increase.
Comorbid conditions [12,20,21]
1. Since, it is a type of fear (if it is rationale/ explained fear of object), we will term it phobia.
2. In Panic, 2nd stress is very prominent, manipulation of 2nd stress is possible, (simply by avoiding it), and feasible and also specific to panic (because avoidance is specific to panic) (* Remember 1st stress is not specific 2nd stress is clinical features of panic=very specific) This avoidance can lead to substance use or OCD (Avoidance will become compulsion which will manifest as REM)
3. All the disorders which fall under the spectrum like stressor related disorder can also be present. AGE: early onset [12].
Not in mid ages because by this time people know that everything can be controlled So in these ages rather than panic, GAD will develop (because they tend to have some control) Good prognosis: Premorbid conditioning is healthy
 So, there is ease of psychotherapy
So, there is ease of psychotherapy
Drugs
As we can see that the noise in brain can be cut by benzodiazepenes and SSRI and Tricyclic antidepressants can be used to maintain levels of SE/NE from falling down in order to be able to initiate an attack of panic, these can be given in disorder [12].
Phobia
1. Manipulation of stress not possible.
2. Person ‘wants to control’ stress.
3. REM mounted.
4. Situation ‘should be’ under control.
5. Situation is presently not under control.
6. Person needs to worry.
7. No control is possible in the situation.
8. Stress can be justified or told.
Interestingly, what may not be justifiable in first setting (diagnosing panic) may become justifiable for 2nd time and thus making it phobia.
Clinical Features
1. Clinical features are similar to panic [12,23].
2. Therefore, stress is justifiable by the person, the features will be specific and that specific will generate features (similar to Koch’s postulate).
3. Onset is similar to panic but can be little controlled.
4. It can be a ‘rational manifestation’ of mood state. So, in order to differentiate it must cross the max period of a mood cycle (i.e. 6 months).
Co-Morbidity
âÞã Stress is justifiable → can be related to stressor related disorder âÞã Avoidance can generate a controlled attack and can lead to development of GAD, because here, patient has some sense of control, while if the person is exposed, the attack will mimic panic attack.
âÞã A constant stress (in those, where stress is a very common thing, like in social phobia) may generate depression if not GAD [12,23,24].
Age
âÞã Secondary to panic.
âÞã First encounter in early age.
âÞã In adulthood → those conditions whose first encounter is in adulthood [3].
Kaplan [12] writes the key aspect of successful treatment are-
I. Patient’s commitment to treatment (developing control).
II. Clearly identifying problems and objectives.
III. Available alternative strategies for coping and feelings.
Treatment
Psychotherapy should include exposure and response preventions OR systemic desensitization, both are in accordance with the diagnosis of etiologic [12,23,25].
Drugs: similar to panic [12,23].
Generalized anxiety disorder
Basic feature
This occurs three times in the chart:
1. When REM has started but manipulation not mount (on stress Law 4s has been applied to end NREM, i.e., psyche is intact and reasonable to some extend but Law 4c is overwhelming and person do not mount manipulation because the same is also disturbing) leading to development of anxiety.
2. When illness is already is already present in the body and person cannot mount a specific manipulation, somatization is not possible and the person has two options:-
a. To submit to psyche progressing to depression spectrum.
b. To fight back which would develop into anxiety.
3. When some control is present in panic → anxiety comes in bouts and gets conditioned (law 4c is active and can exercise some control when body becomes uncontrolled in panic).
I. OCD/Substance abuse/feeding disorder can be present,
II. Can be present with depression spectrum,
III. Can be associated or present with panic/phobia disorder.
1. Stress:- Should be very prominent or should be multiple in number to condition anxiety,
2. Duration criteria- Again to discriminate it with manifestations of REM/NREM cycle, it must complete the whole brain cycle( 6mnts)
3. Individual always wants to exercise control, can even exercise some control i.e. it’s not panic.
4. Features of REM on body and features of fear present.
5. In first two cases, features of somatization can also be present.
Age
This comes when person’s psyche is enough developed to exert sense of control and fear of not being able to control.
So, it would occur most likely in adulthood, but can also occur in middle and old ages, especially IIIrd, in which illness is present [3].
Risk of Suicide
Therefore, if associated with depression spectrum, can do suicide (as GAD in REM disorder) and the risk is potentially high in second form [12].
Psychotheray
Is basically based on finding the stress and using the conditioning present in the patient (most commonly talking is useful).
Therefore, if reason is not present and person’s ‘will’ to control the situation is present, therapy becomes easy if given on time and with proper psychotherapy the prognosis of GAD is very good.
Drugs
Mitigate the immediate effect of REM to reinstate person’s confidence. It can be some with SER inhibitors or BZDs [12,19].
It must be combined with psychotherapy because psychotheray is the ultimate choice.
OCD
1. Persistent thoughts cause conditioning,
2. Psyche overcomes inertia of persistence,
3. Manipulation found specific to stress,
4. Manipulation is feasible to psyche,
5. Conditioning of manipulation.
Clinical Features
Resisting manipulation would mean Law 4 is applied, but Law 4m is being resisted as it has caused second stress

To control both Law 4c is being applied (Remember, here Law 4s cannot be applied as person has already applied it to centre REM) [12,29,30].
1. Manipulation is always in REM because it is specific action. Resisting it would keep the person in REM and transfer the energy to body. This energy on body will produce anxiety like signs and symptoms.
2. Therefore, the person has already applied Law 4s and is trying to find a manipulation for activitywith original rationality; the person may not find a manipulation and will again result in anxiety.
3. In short, almost every disorder can occur with OCD.
4. Schizophrenia can be present if person is obsessed with magical thinking and in compulsion, he gives upto psyche. (like in schizotypal personality person developing schizophrenia)
5. Developing depression spectrum is most likely outcome, as can be seen from the flowchart, the most common rational outcome should be substance use followed by GAD (especially where person is more conscious and substance use is culturally not sanctioned/acceptable, like in females and people who abstain from drinking).
Age
Already discussed, conditioning are most likely to develop in adolescence and early adulthood. So, the age group of 10-25 should be a perfect trap for OCD.
In persons facing less exposure in this period or those facing shocking exposure in mid age can be prone to develop OCD. But as new conditionings are difficult to form in elderlies, it is less likely to have onset in late age group. NEURO: - defect is in “Z” process activation and persistence -→ can be ended by elevating eves of SER/NE [12,31].
Risk of Suicide
If depression spectrum is present, risk should be high theoretically, but not in normal OCD people (those who do not have depression spectrum, OCD is sort of protective against suicide). It can be high in absence of proper conditioning (childhood onset), or in presence of bizarre and delusional thoughts( signs and symptoms similar to psychosis) [12,32].
Duration
It can occur as manifestation of REM/NREM cycles, so, it is better to confirm it after 6 months. Also, depression can co-exist, so it is better to find out if it with/without depression.
Psychotherapy
1. Person knows everything, so giving him insights might be more distressing for him.
2. Rather than focusing on 1st stress, one shall focus on:-
I. Avoidance of 2nd stress
II. Developing conditioning, to bypass anxiety developing out of 2nd stress avoidance/ resistance
3. Along with drugs, (if person prefers) add coping skills.
4. If drugs is not preferred by the person (as the person might become more stressed as daily drug taking can act as 3rd stress for the person)
5. Consider strengthening psyche by exposure and response prevention.
Though, body dysmorphic disorder can be considered a part of OCD, trichotillomania is a bit different and can be seen as non-specific manipulation to tension or earning gratification by it.

Whatever it be, both are disorder of uncontrolled REM

“Z” process can be ended by raising levels of SER/NE (in fact they can also create a sense of gratification, which earlier was gained by activities of compulsion).
Somatization
Aetiology/Diagnosis
1. Stress ïÃÆàpersistent thoughts,
2. Psyche overcomes inertia of persistence
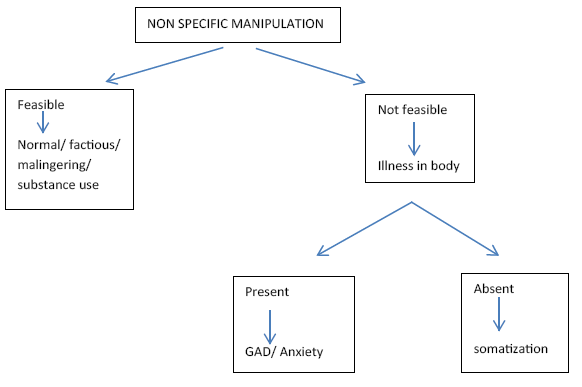
3. Manipulation found ïÃÆànon-specific to stress
4. Manipulation is not feasible for psyche
5. Diagnosed illness usually absent
Clinical Features [12,19,33,34]
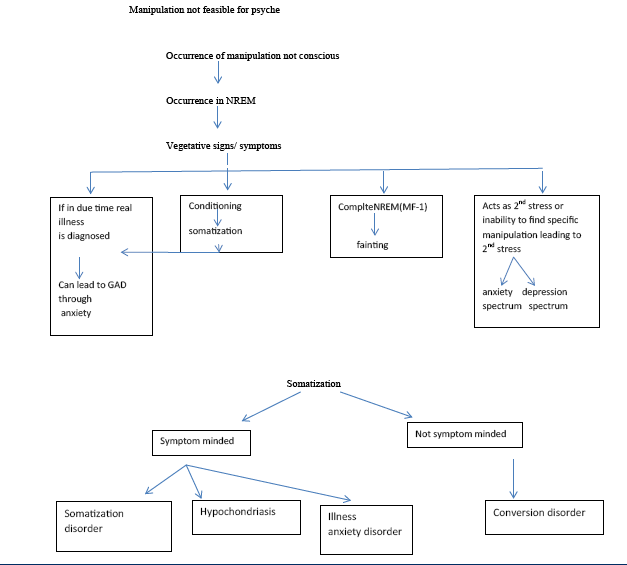
Comorbidities
Clearly evident both anxiety and depression can occur [35].
Age of onset
Earlier for conversion (if the person, manipulation is not possible for psyche → he would try to control manipulation and thus by Law 4c the MF can never be one and conversion cannot occur).
So, in person having better conditioning, especially middle ages, the persons are more likely to make somatization rather than conversion [12].
Risk of suicide
In depression spectrum, otherwise the person is less likely to think of such things.
Pharmacotherapy
1. Treatment of the comorbidities, as here the manipulation is non-feasible and non- specific. So, acts as second stress.
2. Treatment of the symptom even with placebo, if necessary, every step should be taken to assure physician’s help (but not of family) (so that, it remains non feasible only) If the signs and symptoms are more of symptom minded, special care should be taken to stop doctor shopping (so, physicians’ help is must)
3. Therefore , the person has no feasible manipulation, NREM stage is prominent → NREM enders like SSRI should be given
Psychotherapy
1. Here, the need of generating new coping skills is of urgent nature.
2. Feeding of symptoms should be avoided. Ask family not to feed to signs/symptoms(that is don’t give extra care)
3. Avoidance of patient can aggravate the disease, because as per conditioning of patient, illness is a non-specific manipulation to stress, but if that is not taking care of stress, illness is bound to increase. So, do not completely avoid the patient.
4. Elimination of stress → also, as the manipulation is non-specific, usually the stress would be of ‘unspeakable’ nature. So, convince the family and patient that his stress is conversable.
5. Equal treatment of co-morbidities is needed.
(Unlike in dissociation or schizophrenia, treatment is not complex, rather easy but deliberate)
Factitious disorders is similar to somatization except for the fact that person knows the “manipulation” is feasible, usually with no associated co-morbidities. In treatment drug therapy is given accordingly and of course, no psychotherapy is needed for complication. Also, try to convince patient indirectly that manipulation is not good (never directly as then patient will try finding new ones).
Dissociation Disorder
Etiology/diagnosis
1. Stress → persistent thoughts
2. Psyche overcomes inertia of persistence
3. Manipulation found → specific to stress
4. Manipulation is not feasible for psyche
5. Development of at least 2 psyche [12,37-39]
I. Original → which will manifest similar to person who hadn’t found any specific manipulation.
II. Second or further psyche are complementary ones designed for special purpose to cope with specific stress.
Replacement of 1st/original psyche by original one will surely depend upon feasibility of environment can be seen.
Simplest is depersonalization/de realization.
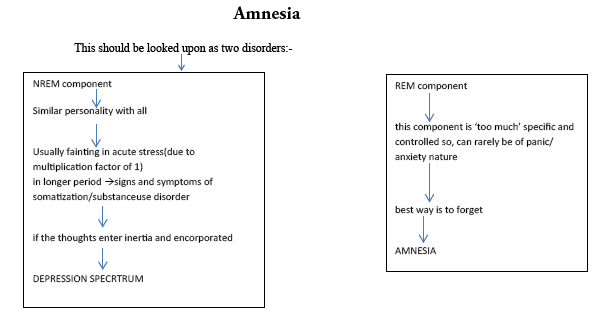
For people, most easy things to perform a manipulation would be to forget it.
NREM → Fainting of 1st psyche
REM → amnesia of 2nd psyche This should be looked upon as two disorders:-
Age group a little higher (person becomes less dramatic with age)
In younger ages → people are more dramatic and they tend to have very dramatic and metaphorical conditioning. (For example avoiding a stress with sunning away from stress- running away)

When first psyche faints → the second will run away → thus, first will never remember how it occurred.
If this conditioning persists, person may become a persistent case of dissociation fugue and may run a lot of times
When the person comes back to normal, he may wish to go back
Most interesting is dissociative identity, here, the manipulation is not an escapist but a fighter usually and the second personality is specially designed to cope up with special conditions.
Therefore, here the 2nd psyche is not just complementary but has a distinct personality subjugation to 2nd psyche as will occur in dissociation can be equated to giving up of pschye in schizophrenia.
Therefore, it is more like giving up to psyche. This 2nd psyche is very strong, schizophrenia like signs/symptoms may develop and even persist it given chance to.
In Depersonalization/Derealization → The trauma is not that significant to induce 1X multiplication factor for NREM, so, while the first remain intact, the 2nd psyche takes its place.
Remember, in this 2 psyches are co-existing but not actively controlling brain cycle. While the 2nd psyche is dominant for some time (manipulation), the 1st psyche still has control and is continued. Therefore, the NREM is being manipulated, usually the 2nd psyche should be lucid, but it can be violent if the conditioning permits. What so ever it be, it won’t be active in real world because the person is still in NREM only. so, basically this is not even a true dissociation because both psyches are in same state.
Theoretically speaking, the youngest age of onset should be of dissociation identity disorder (because of increased conflicts in childhood and early adulthood) followed by fugue. The other two have more chances of having an adult onset as they are of more ‘understanding nature’.
Risk of Suicide
Here, risk of depression spectrum is present; risk of suicide is also present.
Also there is an added risk of dissociation. As the 2nd psyche, it can take any form (as it is unchecked by rational conditioning related to available psyche [40].
Drugs
Therefore, the disease has a compulsory NREM portion (one psyche faints or atleast becomes silent.
Best way is to initiate NREM overcoming drugs=SSRI.
Psychotherapy
One of the most difficult to treat but the key to treatment is in weakness of 1st psyche and strength of 2nd psyche.
To strengthen 1st:-
i. Talk about stress,
ii. Develop coping skills,
iii. Develop new and strong conditioning,
To weaken 2nd:-
i. Reduce the significance of 2nd psyche in eyes of 1st psyche one of the most common method that could be practiced is telling family members not to pay heed to 2nd psyche when occurs (similar to that in pseudo seizure).
The most crucial step of any psychiatric problem would be elimination or stress and related conditioning but in dissociation, we have to pay more focus on developing new conditionings.
To develop new conditioning, as mentioned in the principle of conditioning
In this already a conditioning of coping is present, so the 2nd one shall be practiced to change coping skill and 1st one to add new ones (so, that chance of reverting back to dissociation is minimized)
Schizophrenia
Diagnosis/etiology
As already discussed
So, should include
1. Stress → persistent thoughts,
2. Inertia of persistence overcomes psyche
3. Cannot control inertia of REM
4. Gives upto NREM (risk factors discussed)
Clinical features
Depending upon psyche’s maturity (defines age and type)
1. Most mature → catatonia (Later onset); person is not entering REM but over controlling NREM and sometimes counter parts REM.

No need to end REM (no need to off REM)
Immediate need to end the conditioning and that is making him over control (Law 4) Also, NREM should not be abruptly ended → can lead to dangerous REM
No need to find stress → as stress is least important in development of schizophrenia
Remember, if stress is more important → Depression spectrum
If alternative is more important → schizophrenia
This may seem similar to dissociation sprectrum but there manipulation was not feasible.
So, it could come only when 1st psyche fainted. Here the person, assertly ends the 1st psyche to live in 2nd.
2. Most primitive → less conditioning present

Simple
Only negative signs and symptoms
Difficult to treat because
a) Less conditioning → less use of Psychotherapy.
b) REM is not present. So, REM enders not effective (unless, person is being actively simple in REM also) → the likelihood is less than 50% (as REM is never more than 50%) [12,19].
3. REM present
Person has some conditioning of maturity left (so, usually later onset of all)
Paranoid
More likely to respond to psychotherapy and pharmacotherapy
âÞã REM present (early age)
Less conditioning that could maintain maturity in new psyche
Dis-organized thoughts and actions
Therefore, actions are also involved; they are more likely to get conditioned through implicit memory
Development of alternate psyche (personality)
Less likely to respond to psychotherapy [3,30]
4. Therefore, the second psyche is of choice, most likely it is mixed nature and left undifferentiated.
Risk of suicide
Least in catatonics.
Most in simple and paranoid (because some psyche left to mount NREM) [12].
Duration
To be schizophrenia (total new psyche, one must pass both phases of brain cycle with maximum “MF”, so it should be 6 months [12].
The manifestation however can also just be in one phase and thus less than 3 months duration [42].
Co-morbiditie
Anything (as it is personal choice). Will depend upon risk factors [12,43].
Prognosis
Poorer in those with
a. Less conditioning.
b. Overtake by alternate psyche completely.
c. If treated only during disease.
Treatment
a. Similar to dissociation.
b. Eliminate risk factors.
c. No need to focus on stress.
Specially treat the normal individual with psychotherapy and diseased state with pharmacotherapy [12,44].
âÞã To reinstate normal psyche, a good environment is must. The person should be made aware of profits of being normal and losses of being abnormal in terms of his conditioning.
âÞã It is always better not to give generalized treatment but individualize heavily due to fascinating nature of disease.
âÞã Treatment of co-morbidities is second priority unless they are becoming stressful for first psyche.
âÞã If it is for second psyche → prefer not to treat (as it will help in psychotherapy).
Conclusion
Though most of the paper concludes what we already know but now with a better understanding and evidently with one single model, however it might be comfortable if we revisit some points that are theoretically novel and possible:
Fear is good, fight is good and fright is also good because all these lead to increased conditionings and can yield better clarity of thoughts unless you get to much involved and rather than making REM active it ultimately activates the NREM for protection purposes
An already ill patient is more unlikely to develop somatization spectrum and more likely to develop generalized anxiety and panic disorders. Schizophrenia is more concerned with psyche’s inability to mount a controllable response so unlike other diseases, stress should not become the center of psychotherapy. In fact the center should be to modify patient’s environment (resisting new one and endorsing old one but interestingly)
In depression and dysthymia drug can do more benefit because the psyche is not able to activate the serotonergic or noradrenergic pathways, while in neurosis the psyche is able to mount a response so drugs would not be that effective as the psychotherapy would be.
A disorder is more likely to have co-morbidities in the spectrum it is falling like substance use disorder, feeding disorder and OCD fall in one spectrum and thus patient is likely to have more than one of it at time of diagnosis
Thus we can prove on basis of above explanation and explanation for psychiatric disorders as attached with supplement that there can be a single model which could elaborate the disorders of psychiatry including risk factors, criteria for diagnosis, age of onset, duration, clinical features, co-morbidities, risk of suicide, prognosis and attempting to formulate the rationale basis for both pharmaco and psychotherapies, thus proving our alternate hypothesis on basis of my hypothetical model
The scope of paper lies in its implication. For this paper implications are:
Establishing diagnostic criteria for diseases which will be specific so that no two diseases are to be confused with even with overlapping symptoms Finding out risk factors and co-morbidities based on principles and algorithm
Implementation of better psychotherapy as reaching cause will be easier by algorithm Predicting duration of illness and thus the natural course of time for which drug administration shall be rational in a given disease.
Predicting prognosis individually especially in those cases where prognosis is often complicated by risk of suicide.
These are the things that can be well predicted along with many normal phenomena like while we sometimes feel sleepy in a day and don’t want to do work (because during that time we are in NREM so by principle of inertia the brain will guide psyche to formulate actions to keep itself in same so we also find out reasons to sleep and also convince us during that time that it would be better to sleep) and why we sometimes feel too fresh and energetic (due to REM). There is much normal human behaviour that can be explained by this phenomenon but enlisting them all is out of scope of this paper. Similarly, we can explain each and every fact known of a certain disease (I have tried to explain in the supplement as many as I can in this paper keeping in view limitations of space). Further research can be done to find out multiplication factor for each disease which will help us to limit the overuse of drugs and even psychotherapy! Further, principle of neurotransmission can impart a vector quantity to the research in finding biological markers related to diseases.
Implementation of the diagnostic criteria can further strengthen the spirit of DSM-5 and in new diagnostic authorities biochemical profiles can also be included as David Kupfer says, “… biological and genetic markers that provide precise diagnoses that can be delivered with complete reliability and validity are still disappointingly distant. We’ve been telling patients for several decades that we are waiting for biomarkers. We’re still waiting…”
The wait seems to be over.
Acknowledgements
Expression of gratitude can in no way repay the amount of support and cooperation I have received to complete this project. First thanks to my mother and father for making me able to write this paper and next to the Almighty who blessings bestowed me with capability to come up with the ideas. I would like to thank my sisters Priyanka Di and Prabha Di and elder brother Dr. Jiwesh for their constant motivation and help. I would also like to extend my sincere gratitude to my brother-in-law Dr. Ravi Prakash for his special guidance in writing this paper. I would also like to extend my gratitude to Manmohan Pandey for his constant appreciation. I would also like to thank my grandparents for their unconditional blessings. Last but not the least I would like to thank all my friends whose constant motivation made this path easy and especially Dr. Kirti for her valuable time in keeping the flame burning and reviewing of the project. Thank you everyone and pardon me if I missed someone!
References
- Diagnostic and statistical manual of mental disorders (5th edtn). American Psychiatric Association (2013).
- Foulkes D. Children's dreaming and the development of consciousness. Cambridge: Harvard University Press. (1999).
- Domhoff GW. Moving Dream Theory Beyond Freud and Jung. Paper presented to the symposium "Beyond Freud and Jung?" (2000).
- Abel B. The dream content of menopausal women: An exploratory study. Ph.D Thesis, United States International University, San Diego. (1994).
- Giambra L, Jung R, Grodsky A. Age changes in dream recall in adulthood. Dreaming 6(1), 17-31 (1996).
- Schredl M, Morlock M, Bozzer A. Childhood memories and adult dreams. Z. Psychosom. Med. Psychoanal 42(1), 25-33 (1996).
- Hall C. A cognitive theory of dream symbols. J. of. General. Psychology 48(1), 169-186 (1953a).
- Lakoff G. How unconscious metaphorical thought shapes dreams. In D. Stein (Ed.), Cognitive Science and the Unconscious. Washington: American Psychiatric Press 89-120 (1997).
- Kahan TL. “Measuring dream self-reflectiveness: a comparison of two approaches” Dreaming 4(3), 177-193 (1994).
- Foulkes D. Dreaming: A Cognitive-Psychological Analysis. Hillsdale, NJ: Lawrence Erlbaum (1985).
- Altevogt BM, Colten HR eds. Sleep disorders and sleep deprivation: an unmet public health problem. National Academies Press (2006).
- Sadock BJ, Sadock VA. Kaplan and Sadock Synopsis of psychiatry: Behavioral sciences/clinical psychiatry. Lippincott Williams & Wilkins. (2011).
- Barrett KE. Review of Medical Physiology, 25/e (2010).
- Hudspeth AJ, Jessell TM, Kandel ER, et al. Principles of neural science. McGraw-Hill, Health Professions Division (2013).
- Monti JM, Monti D. Role of dorsal raphe nucleus serotonin 5-HT1A receptor in the regulation of REM sleep. Life. Sciences 66(21), 1999-2012 (2000).
- Roy B, Schmeichel J, Brandon & Vohs, et al. Self-regulation and the executive function: The self as controlling agent. American Psychological Association (2019).
- Eccles, John C. How the Self Controls its Brain. Springer (1994).
- Lewis MD, Todd RM. The self-regulating brain: Cortical-subcortical feedback and the development of intelligent action. Cognitive Development 22(4), 406-430 (2007).
- Ahuja N, Niraj A. A short textbook of psychiatry. Jaypee Brothers Publishers (2011).
- Craske MG, Waikar SV. Panic disorder. Handbook of prescriptive treatments for adults. Psychology 135-155(1994).
- Leckman JF, Weissman MM, Merikangas KR, et al. Panic disorder and major depression: Increased risk of depression, alcoholism, panic, and phobic disorders in families of depressed probands with panic disorder. Arch. Gen. Psychiatry 40(10), 1055-1060 (1983).
- Gould RA, Ott MW, Pollack MH. A meta-analysis of treatment outcome for panic disorder. Clin. Psychol. Rev 15(8), 819-844 (1995).
- Heimberg RG. Social phobia: Diagnosis, assessment, and treatment. Guilford Press (1995).
- Essau CA, Conradt J. Petermann F. Frequency and comorbidity of social phobia and social fears in adolescents. Behav. Res. Ther 37(9), 831-843 (1999).
- Barlow DH, Craske MG, Cerny JA, et al. Behavioral treatment of panic disorder. Behav. Ther 20(2), 261-282(1989).
- Rowa KAREN, Antony MM. Generalized anxiety disorder. Psychopathology: History, diagnosis, and empirical foundations. 78-115 (2008).
- Lader M. Generalized anxiety disorder. In Encyclopedia of Psychopharmacology (pp. 699-702). Springer Berlin Heidelberg (2015).
- Newman MG. Generalized anxiety disorder. Effective brief therapies: A clinician’s guide, pp.157-178.(2000)
- Riggs DS, Foa EB. Obsessive-compulsive disorder. Comprehensive Handbook of Personality and Psychopathology 169(1), (1993).
- Grant JE, Obsessive–compulsive disorder. N. Engl. J. Med 371(7), 646-653 (2014).
- Abramowitz JS, Taylor S, McKay D. Obsessive-compulsive disorder. The. Lancet 374(9688), 491-499. (2009).
- Torres AR, Ramos-Cerqueira AT, Ferrão YA, et al. Suicidality in obsessive-compulsive disorder: prevalence and relation to symptom dimensions and comorbid conditions. J. Clin. Psychiat 72(1), 17-26 (2011).
- Mai F. Somatization disorder: a practical review. Can. J. Psychiatry 49(10), 652-662 (2004).
- Lipowski ZJ. Somatization: the concept and its clinical application. Am. J. Psychiatry 145(11), 1358-1368. (1988).
- Smith GR. The epidemiology and treatment of depression when it coexists with somatoform disorders, somatization, or pain. Gen. Hosp. Psychiatry 14(4), 265-272 (1992).
- Kroenke K. Efficacy of treatment for somatoform disorders: a review of randomized controlled trials. Psychosom. Med 69(9), 881-888 (2007).
- Chu JA, Frey LM, Ganzel BL, et al. Memories of childhood abuse: Dissociation, amnesia, and corroboration. Am. J. Psychiatry 156(5), 749-755 (1999).
- Kluft RP. Dissociative disorders. In Handbook of aggressive and destructive behavior in psychiatric patients 237-259 (1994).
- Howell EF. Understanding and treating dissociative identity disorder: A relational approach. Routledge. (2011).
- Foote B, Smolin Y, Neft DI, et al. Dissociative disorders and suicidality in psychiatric outpatients. J. Nerv. Ment. Dis 196(1), 29-36 (2008).
- International Society for the Study of Trauma and Dissociation, Guidelines for treating dissociative identity disorder in adults, third revision. J. Trauma. Dissociation 12(2), 115-187 (2011).
- Tsuang MT, Winokur G. Criteria for subtyping schizophrenia: Clinical differentiation of hebephrenic and paranoid schizophrenia. Arch. Gen. Psychiatry 31(1), 43-47 (1974).
- Fenton WS. Comorbid conditions in schizophrenia. Curr. Opin. Psychiatry 14(1), 17-23 (2001).
- Lehman AF, Lieberman JA, Dixon LB, et al. Practice guideline for the treatment of patients with schizophrenia. Am. J. Psychiatry 161 (2 SUPPL.) (2004).